Breaking Free from Steroid Dependence? Frontier Advances in Autoimmune Hepatitis
Autoimmune hepatitis (AIH) is a chronic inflammatory liver disease in which the immune system mistakenly attacks the body's own hepatocytes, leading to liver cell damage, inflammation, fibrosis, and potentially progressing to cirrhosis or liver failure. It can occur at any age, in any race or gender, but is markedly more common in females (female:male ratio ≈ 3–4:1), with a global prevalence of about 10–25 per 100,000. It is classified into type 1 (most common, associated with ANA and/or SMA positivity, often coexisting with other autoimmune diseases) and type 2 (less common, mainly in children, associated with anti-LKM1 or anti-LC1 positivity). Diagnosis relies primarily on elevated serum transaminases, hypergammaglobulinemia (especially IgG), positive autoantibodies, liver histology showing interface hepatitis with plasma cell infiltration, and exclusion of viral hepatitis, drug-induced liver injury, and other causes. Without treatment, it can be fatal, but immunosuppressive therapy (e.g., glucocorticoids + azathioprine) usually induces remission and improves survival.
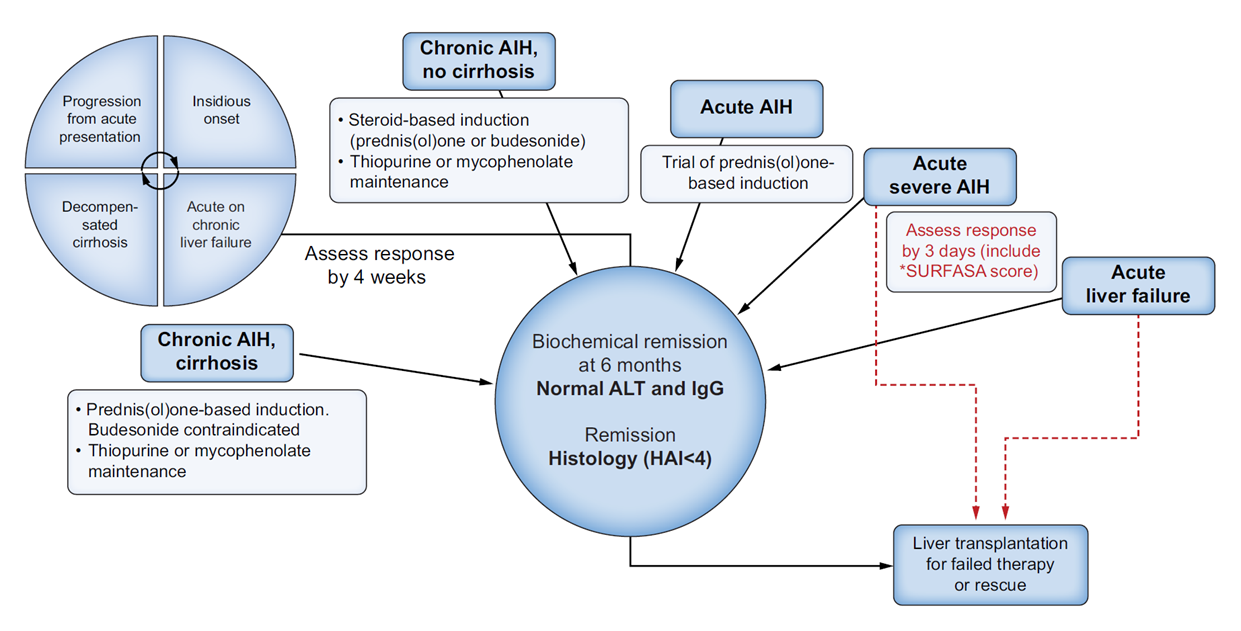
Figure 1. Spectrum and management options in autoimmune hepatitis
Pathogenesis
AIH pathogenesis is driven by a combination of genetic susceptibility, environmental triggers, and breakdown of immune tolerance, with the core being autoimmune attack specifically targeting hepatocytes: Susceptibility genes such as HLA-DR3/DR4 lay the foundation for immune dysregulation; environmental factors like viral infections, drugs, or gut dysbiosis disrupt tolerance; dendritic cells present liver autoantigens (e.g., CYP2D6, SLA/LP), activating Th1/Th17 CD4+ T cells that release pro-inflammatory cytokines (IFN-γ, TNF-α, IL-17) to directly induce hepatocyte apoptosis. Concurrently, reduced numbers or functional defects in regulatory T cells (Tregs) fail to suppress excessive effector T-cell responses. B cells produce autoantibodies that further amplify liver inflammation. Molecular mimicry of foreign antigens initiates autoimmunity, while gut-liver axis dysregulation promotes antigen leakage and sustained immune activation. Chronic inflammation activates hepatic stellate cells, ultimately driving liver fibrosis progression.
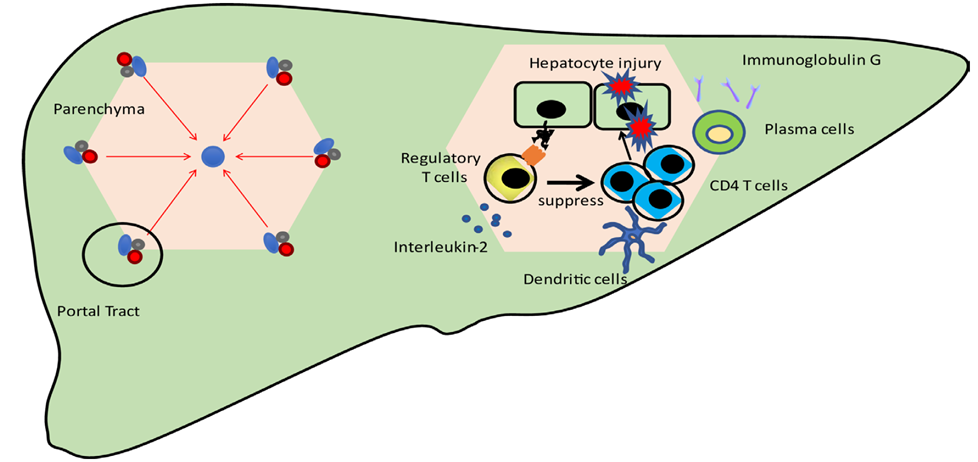
Figure 2. Overview of pathogenesis
Core Clinical Features
Symptoms: Early disease is often asymptomatic or presents with nonspecific symptoms such as fatigue, anorexia, jaundice, or right upper quadrant discomfort. Acute flares can rapidly progress to liver failure, with severe fatigue, coagulopathy, hepatic encephalopathy, etc.
Laboratory findings: Key abnormalities include markedly elevated serum transaminases (ALT/AST), elevated IgG levels, and positive autoantibodies (e.g., antinuclear antibody ANA, anti-smooth muscle antibody SMA, anti-liver kidney microsomal type 1 anti-LKM-1, anti-soluble liver antigen/liver pancreas SLA/LP). SLA/LP has relatively high specificity for AIH, while others lack organ specificity.
Histological features: Liver biopsy shows interface hepatitis and portal tract plasma cell infiltration — the hallmark distinguishing AIH from other chronic liver diseases.
Based on autoantibody profile, it is divided into two types:
Type 1: ANA/SMA positive, accounting for 60%–80% of AIH cases.
Type 2: anti-LKM-1 positive, more common in children and young adults, with relatively faster progression.
Some patients present with AIH-PBC overlap syndrome, requiring integrated clinical, laboratory, and pathological evaluation for differentiation.
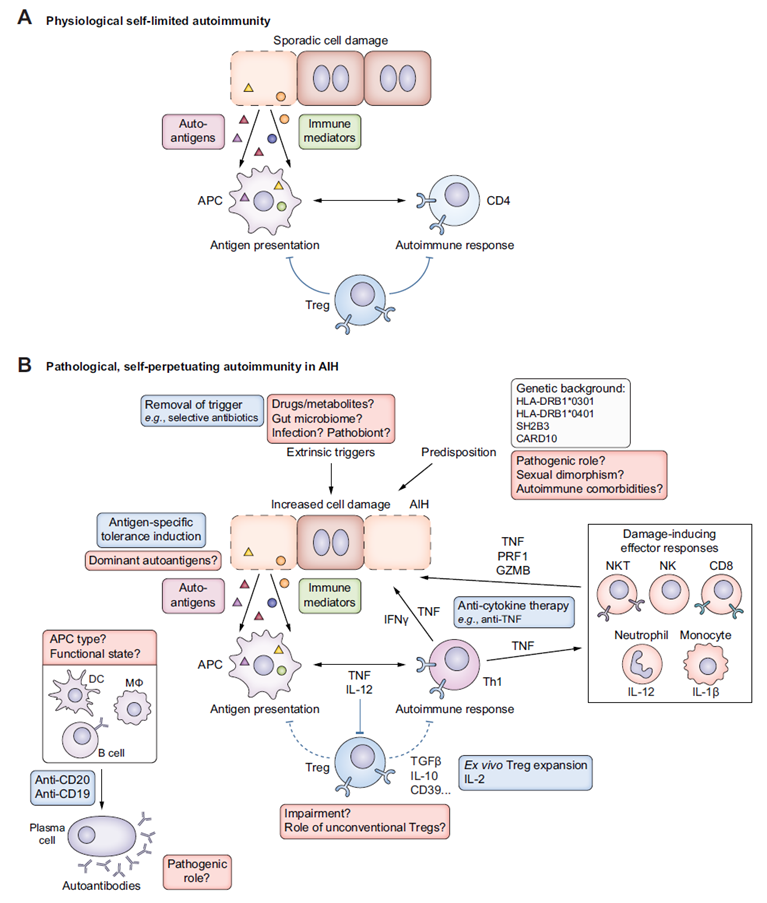
Figure 3. Immunopathology of autoimmune hepatitis and potential therapeutic strategies
Frontier Research Advances and Key Targets
B-Cell-Targeted Therapies
BAFF blockade has emerged as a major breakthrough for refractory AIH. BAFF (B-cell activating factor) is a key cytokine that supports B-cell survival, plasma cell differentiation, and antigen presentation. In AIH patients, serum BAFF levels are significantly elevated, promoting both B-cell/plasma cell function and Th1/Th17 differentiation while suppressing Treg generation, creating a vicious immune cycle. Blocking the BAFF receptor not only depletes B cells but also interrupts this amplification loop, making it one of the most promising third-line/refractory targets. Leading candidates include ianalumab (VAY736, anti-BAFF receptor monoclonal antibody) (NCT03217422, ongoing Phase 2/3 randomized double-blind placebo-controlled trial in refractory/intolerant AIH patients) and Belimumab (anti-BAFF monoclonal antibody) (NCT06381453, currently recruiting, evaluating steroid-sparing potential and safety when added to standard therapy; small-sample data suggest effective control of active AIH and improvement in steroid dependence).
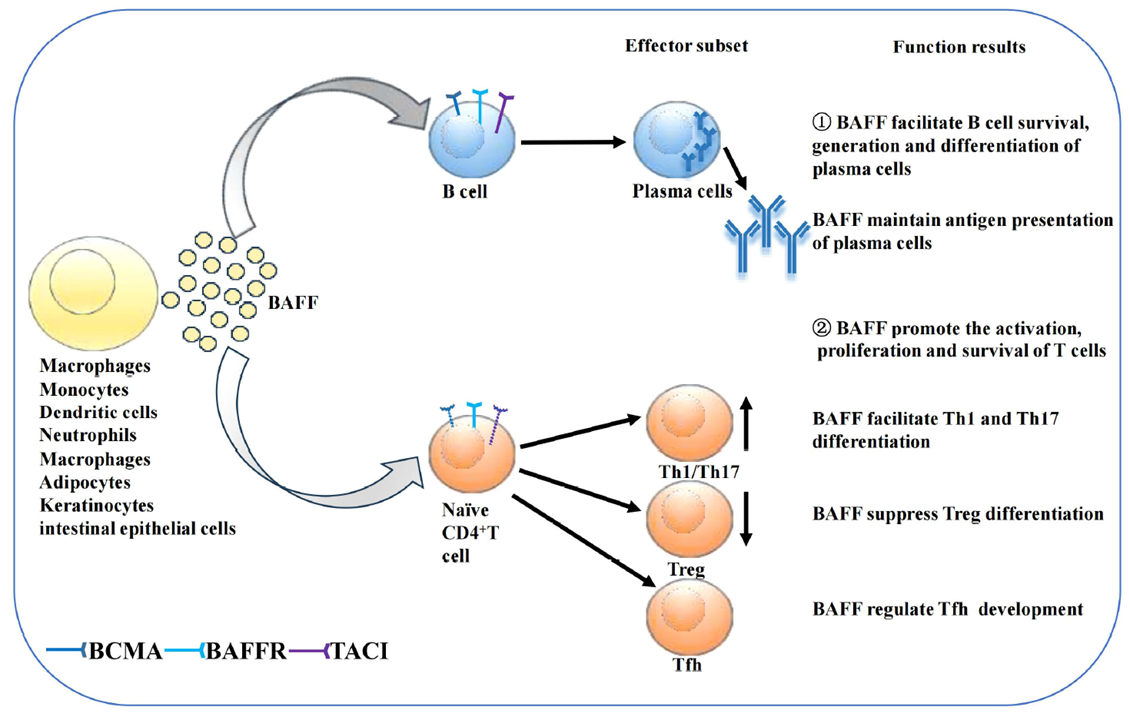
Figure 4. Effects of BAFF on B cells and T cells
Gut Microbiome and Metabolites
Gut dysbiosis promotes Th17 dominance and Treg suppression. Microbial metabolites such as short-chain fatty acids (e.g., butyrate) and secondary bile acid derivatives (e.g., 3-oxoLCA inhibits RORγt, isoalloLCA enhances Foxp3) regulate Treg/Th17 balance and show protective effects in AIH models. Fecal microbiota transplantation or targeted metabolite interventions represent emerging directions.
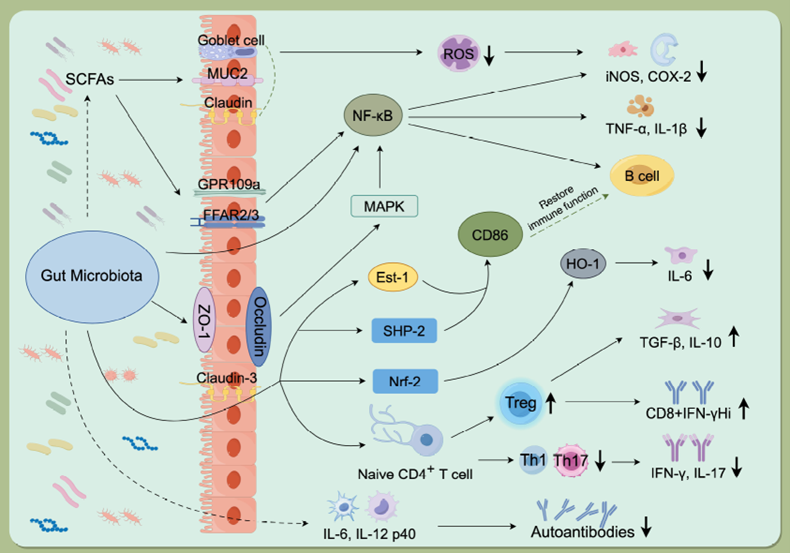
Figure 5. Mechanisms of gut microbiota involvement in autoimmune diseases
Other Emerging Mechanism-Targeted Therapies
Immunoproteasome inhibitors: zetomipzomib (KZR-616) selectively inhibits the immunoproteasome, modulating inflammatory antigen processing and pro-inflammatory cytokine production. The PORTOLA Phase 2a trial (NCT05569759) has been completed, demonstrating favorable safety and steroid-sparing biochemical remissions. In January 2026, the FDA granted Kezar Life Sciences a Type C meeting to discuss the design of a potential global Phase 2b study in refractory/relapsed AIH, marking progress toward later-stage clinical validation of this first-in-class immunoproteasome-targeted agent.
Low-dose IL-2: Selectively activates high-affinity CD25+ Tregs to restore immune tolerance. Preliminary data from compassionate use cases and preclinical models suggest potential for normalization of liver enzymes and IgG levels, though controlled clinical evidence in AIH remains limited. Multiple randomized trials in other autoimmune diseases (e.g., SLE, type 1 diabetes) support further investigation of this approach in AIH.
Metabolomics + nanodelivery: LC-MS identifies AIH-specific metabolic profiles (abnormalities in amino acids, lipids, bile acids) for early diagnosis and prognostic stratification; nanocarriers enable precise delivery of the above targeted agents, reducing systemic side effects.
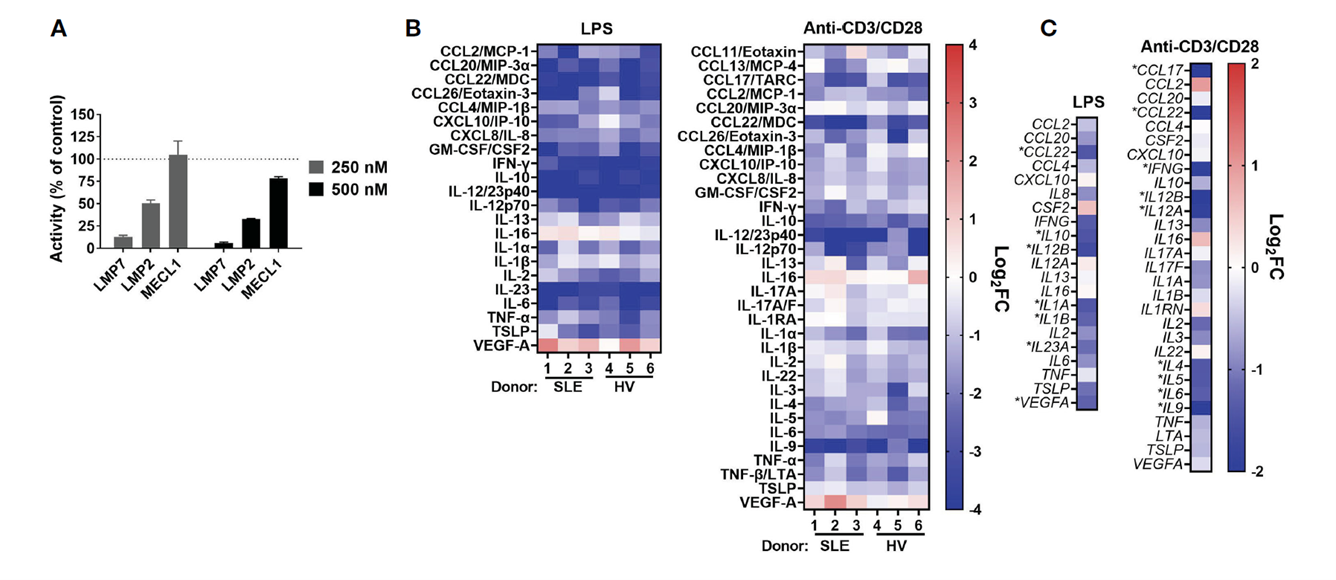
Figure 6. KZR-616 selectively inhibits the immunoproteasome and blocks cytokine production in human PBMCs
First-line treatment remains glucocorticoid induction (e.g., prednisone or budesonide) plus azathioprine maintenance, aiming for biochemical remission (normalization of liver enzymes and IgG) and histological improvement. However, 10%–20% of patients experience non-response, loss of response, or intolerance (e.g., bone marrow suppression, pancreatitis). Long-term steroid use causes significant adverse effects (osteoporosis, diabetes). These targets and guideline updates signal a transition in AIH therapy from "lifelong steroid dependence" to "mechanism-based precision, steroid-free, and microbiome-metabolite combination" approaches.
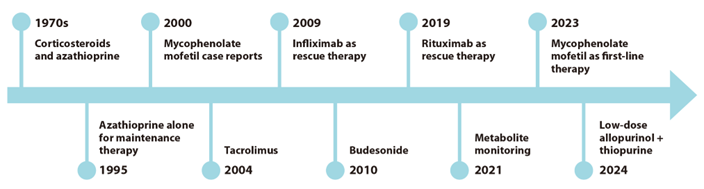
Figure 7. Timeline of autoimmune hepatitis treatments
abinScience Related Products
The following are abinScience's latest recombinant proteins and antibodies relevant to autoimmune hepatitis research, covering key targets discussed in this article including BAFF/BLyS pathway, Th1/Th17 effector cytokines, Treg-associated molecules, and AIH autoantigens. Catalog numbers link directly to the product pages.
Protein
| Catalog No. |
Product Name |
| HF974012 |
Recombinant Human HLA-DRB1 Protein, N-His |
| HY091012 |
Recombinant Human CYP2D6 Protein, N-His |
| HF652012 |
Recombinant Human FTCD Protein, N-His |
| HF996011 |
Recombinant Human CD25/IL2RA Protein, C-His |
| HF996012 |
Recombinant Human CD25/IL2RA Protein, N-His-KSI |
| HF879012 |
Recombinant Human TNFa/TNF-alpha Protein, N-His |
| HW405012 |
Recombinant Human IFNGR2 Protein, N-His |
| HC549012 |
Recombinant Human STAT4 Protein, N-His |
| HT425012 |
Recombinant Human AIRE Protein, N-His-SUMO |
| HF564011 |
Recombinant Human CD275/ICOSLG Protein, C-His |
| HV649012 |
Recombinant Human SH2B3 Protein, N-His |
| HY422012 |
Recombinant Human CD28 Protein, N-His |
| HB651012 |
Recombinant Human CD152/CTLA4 Protein, N-His |
| HB782012 |
Recombinant Human CD40/TNFRSF5 Protein, N-His |
| HW351012 |
Recombinant Human RORC/NR1F3/RORγt Protein, N-His |
View remaining Protein products
Antibody
| Catalog No. |
Product Name |
| HV599016 |
Anti-Human BAFFR/TNFRSF13C Reference Antibody (Ianalumab, RUO) |
| HV212016 |
Anti-Human BAFF/BLyS/TNFSF13B Reference Antibody (Belimumab, RUO) |
| HV212026 |
Anti-Human BAFF/BLyS/TNFSF13B Reference Antibody (Tabalumab, RUO) |
| HS856106 |
Anti-Human IL17A & TNFSF13B Bispecific Reference Antibody (Tibulizumab, RUO) |
| HF564016 |
Research Grade Prezalumab |
| HB782016 |
Research Grade Iscalimab |
| HB782026 |
Research Grade Bleselumab |
| HF879036 |
Research Grade Infliximab |
| HF879046 |
Research Grade Golimumab |
| HF879056 |
Research Grade Afelimomab |
| HF879066 |
Research Grade Nerelimomab |
| HF879076 |
Research Grade Placulumab |
View remaining Antibody products
Kit
Looking for AIH Research Tools?
abinScience provides factory-direct recombinant proteins, antibodies, and ELISA kits targeting BAFF, Treg-associated molecules, AIH autoantigens, and key inflammatory cytokines — with bulk pricing, custom specifications, and technical consultation available.
Email: info@abinscience.com | Tel: +86-27-65523339
References:
1. Mack CL, Adams D, Assis DN, et al. Diagnosis and Management of Autoimmune Hepatitis in Adults and Children: 2019 Practice Guidance and Guidelines From the American Association for the Study of Liver Diseases. Hepatology. 2020;72(2):671-722. doi: 10.1002/hep.31065
2. European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Autoimmune hepatitis. J Hepatol. 2015;63(4):971-1004. doi: 10.1016/j.jhep.2015.06.030
3. Pape S, Schramm C, Gevers TJG. Clinical management of autoimmune hepatitis. United European Gastroenterol J. 2019;7(9):1156-1163. doi: 10.1177/2050640619872408
4. Dalekos GN, Arvaniti P, Gatselis NK, et al. First results from a propensity matched case control study of Belimumab in patients with autoimmune hepatitis (AIH). JHEP Rep. 2020;2(5):100154. doi: 10.1016/j.jhepr.2020.100154
5. Engel B, Stand S, Taubert R, et al. Belimumab treatment in autoimmune hepatitis and primary biliary cholangitis — a case series. JHEP Rep. 2023;5(4):100691. doi: 10.1016/j.jhepr.2023.100691
6. Kezar Life Sciences. Kezar Life Sciences Announces Regulatory Update on Zetomipzomib Program in Autoimmune Hepatitis. Press release, January 9, 2026. https://ir.kezarlifesciences.com
7. Hang S, Paber D, Thomas PG, et al. Bile acid metabolites control TH17 and Treg cell differentiation. Nature. 2019;576(7785):143-148. doi: 10.1038/s41586-019-1785-z

 中文
中文 English
English 한국어
한국어 日本語
日本語 Español
Español Français
Français Русский
Русский


