Vitiligo: From Pathogenesis to Precision Immunotherapy
Overview of Vitiligo
Vitiligo is an acquired chronic depigmenting skin disorder characterized by well-demarcated white patches on the skin and mucous membranes, primarily caused by the selective loss of melanocytes. The global prevalence is approximately 0.36% (95% confidence interval 0.24–0.54%), affecting around 28 million people (based on 2022 population data). The prevalence rate in adults (0.67%) is higher than in children (0.24%), with no significant gender differences, and the geographical distribution ranges from 0.52% in Central Europe and South Asia to 0.23% in East Asia. According to the classification by the International Vitiligo Task Force in 2023, vitiligo is divided into three types: non-segmental (including generalized, acrofacial, etc.), segmental (usually unilaterally distributed), and mixed types. Unclassified forms include focal and isolated mucosal types.
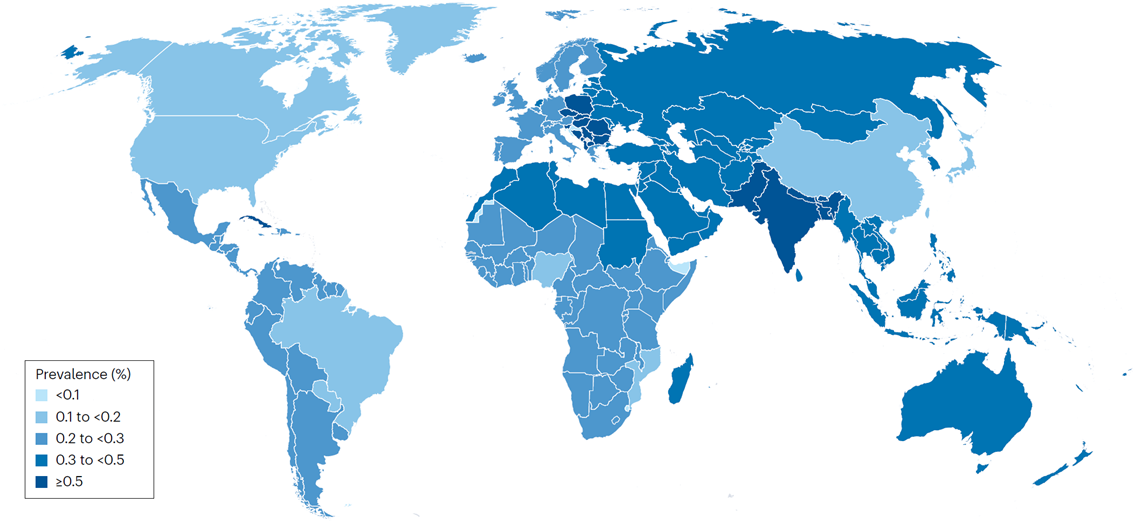
Figure 1. Lifetime prevalence of vitiligo
Clinically, vitiligo often presents as symmetrical depigmented macules, which can affect areas such as the face, extremities, and genitalia. The disease not only impacts appearance but also causes significant psychological burden. A 2022 survey in Europe, Japan, and the United States showed that the self-reported prevalence rate reached 1.3%, among which only 0.6% were diagnosed cases, indicating that many patients do not seek medical help. Vitiligo is often associated with other autoimmune diseases, such as thyroid disorders (approximately 15–25% of patients have concurrent autoimmune thyroiditis).
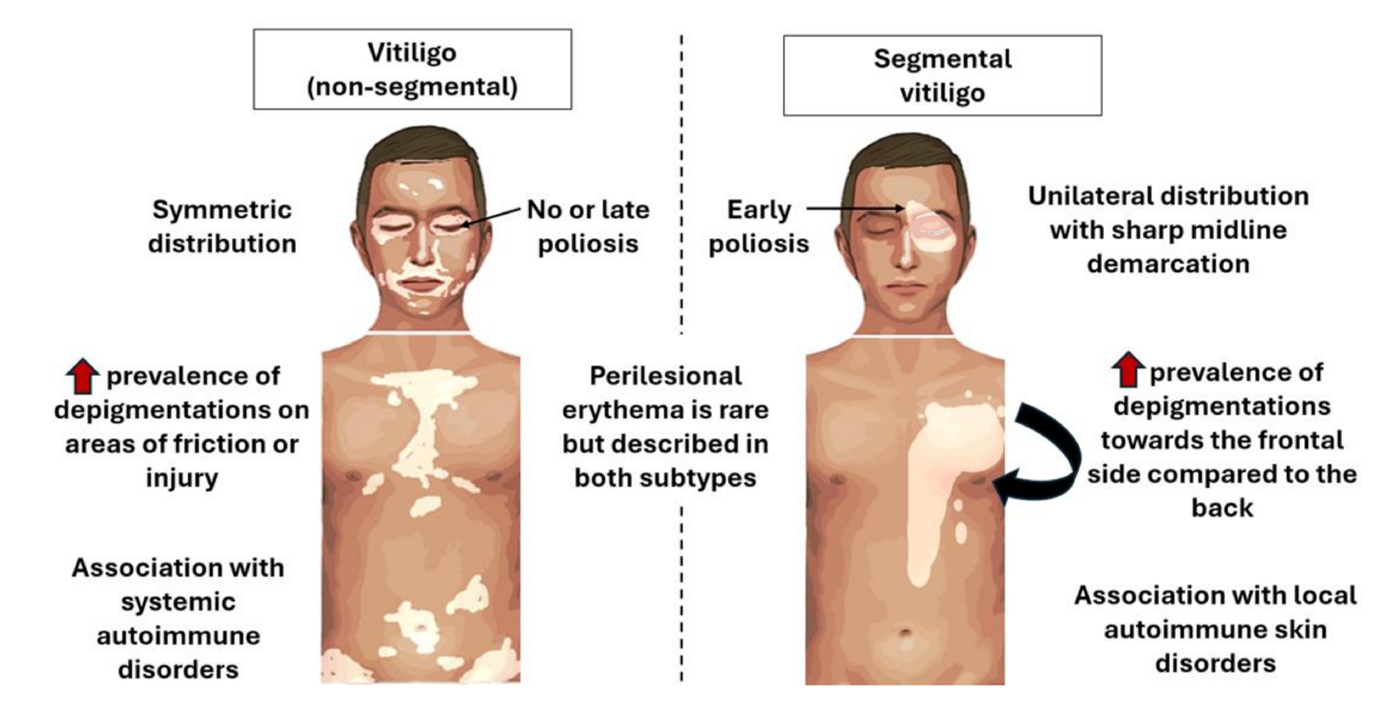
Figure 2. Clinical manifestations of vitiligo (non-segmental type) and segmental vitiligo
Pathogenic Mechanisms
The pathogenesis of vitiligo is complex and involves multiple factors, including genetic susceptibility, oxidative stress, inflammation, and autoimmunity. Traditional views hold that it results from "suicide" or immune attack of melanocytes, but the "convergence theory" integrates these into a comprehensive framework: genetic factors combined with environmental triggers (such as UV exposure, trauma, or chemicals) lead to melanocyte dysfunction.
Genetic factors: Genome-wide association studies (GWAS) have identified approximately 50 susceptibility loci, including genes related to immune regulation such as HLA, TYR (tyrosinase), and genes associated with IFN-γ signaling. There is a strong familial aggregation, with a concordance rate of 23% in monozygotic twins.
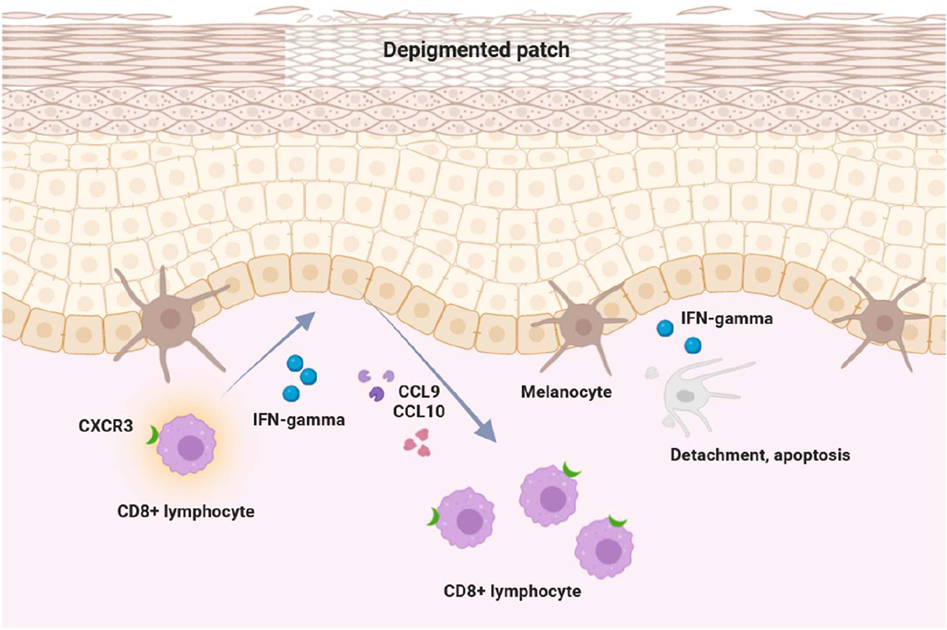
Figure 3. Elucidation of the pathogenesis of vitiligo: the IFN-γ-chemokine axis and its associated positive feedback loop
Oxidative stress: Melanocytes are sensitive to reactive oxygen species (ROS). Mitochondrial dysfunction leads to ROS accumulation, activating endoplasmic reticulum (ER) stress and the unfolded protein response (UPR), ultimately inducing cell apoptosis. Studies have shown decreased catalase activity in the skin of vitiligo patients.
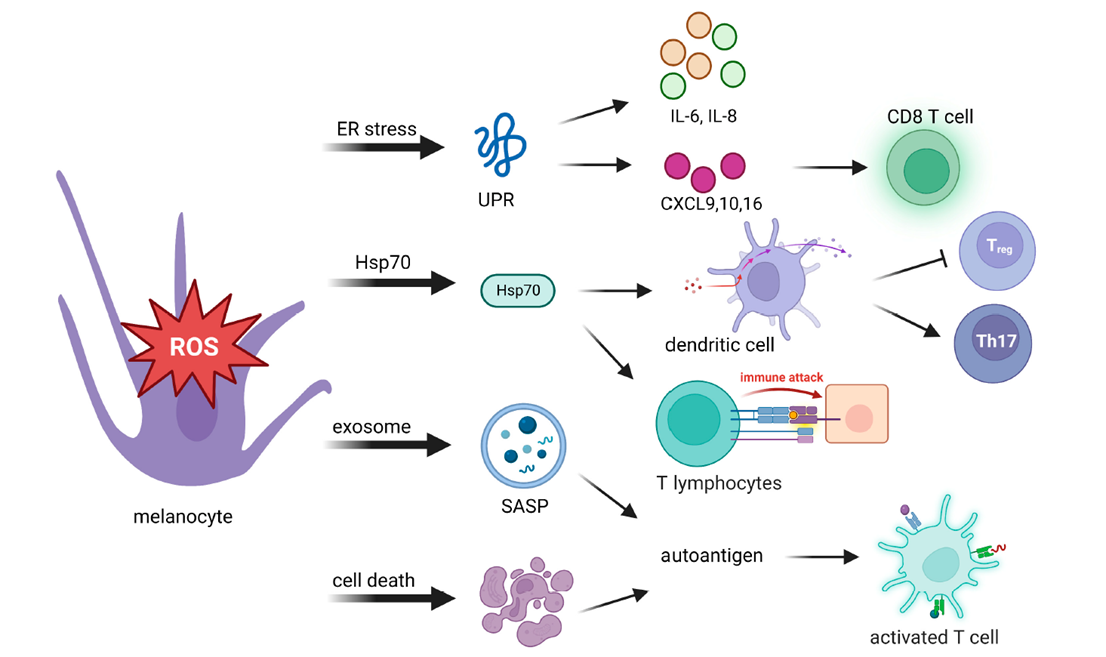
Figure 4. Oxidative stress activates adaptive immunity by presenting self-antigens to the innate immune system
Autoimmunity: The core mechanism involves CD8+ T cell-mediated destruction of melanocytes. IFN-γ signaling activates the JAK/STAT pathway, promoting the expression of CXCL9/10 chemokines, which recruit T cells to form "tissue-resident memory T cells (TRM)." Heat shock protein 70 (HSP70) activates dendritic cells to produce IFN-α, further amplifying the inflammatory cascade.
Other mechanisms: Neural factors (such as catecholamine release) and microbiome dysregulation (such as changes in gut microbiota) may also be involved.
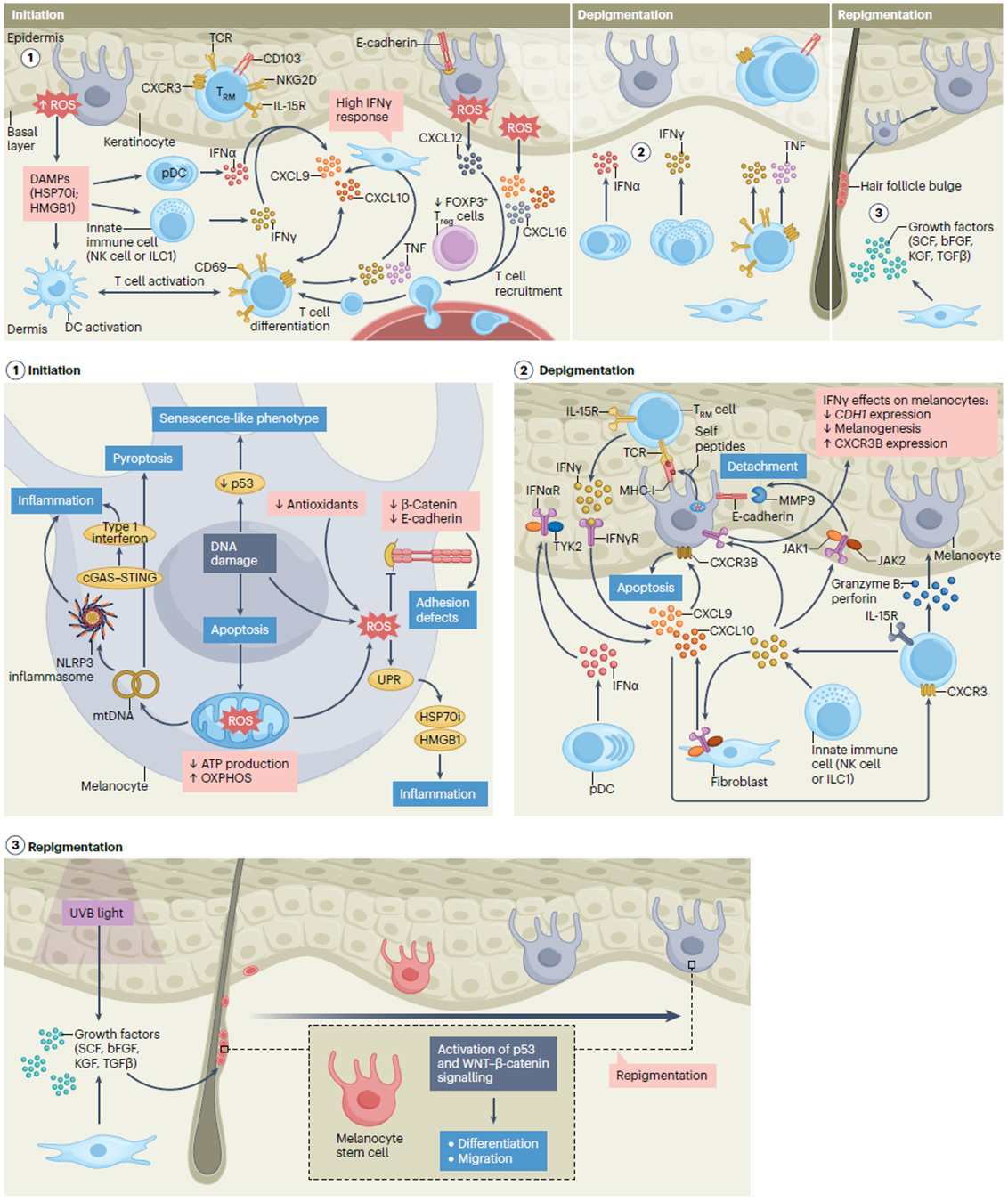
Figure 5. Pathogenesis of vitiligo
Cutting-edge Research Advances
In recent years, vitiligo research has shifted from basic mechanisms to clinical translation, focusing on targeting immunity and melanocyte regeneration. The FDA approval of the topical JAK inhibitor ruxolitinib (Opzelura) in 2022 marked a new era of treatment: a Phase III trial showed that 30% of patients achieved a 75% improvement in facial Vitiligo Area Scoring Index (VASI) at 12 weeks. Other advances include:
AI and digital tools: AI-driven mobile applications enable remote monitoring of disease progression. A 2023 study proposed a CNN (Convolutional Neural Network)-based app using the YOLO architecture to detect lesions with an accuracy of 92.91% and a segmentation Jaccard index of 0.79. Another tool combining Wood's lamp and dermoscopy improved diagnostic consistency (κ = 0.40).
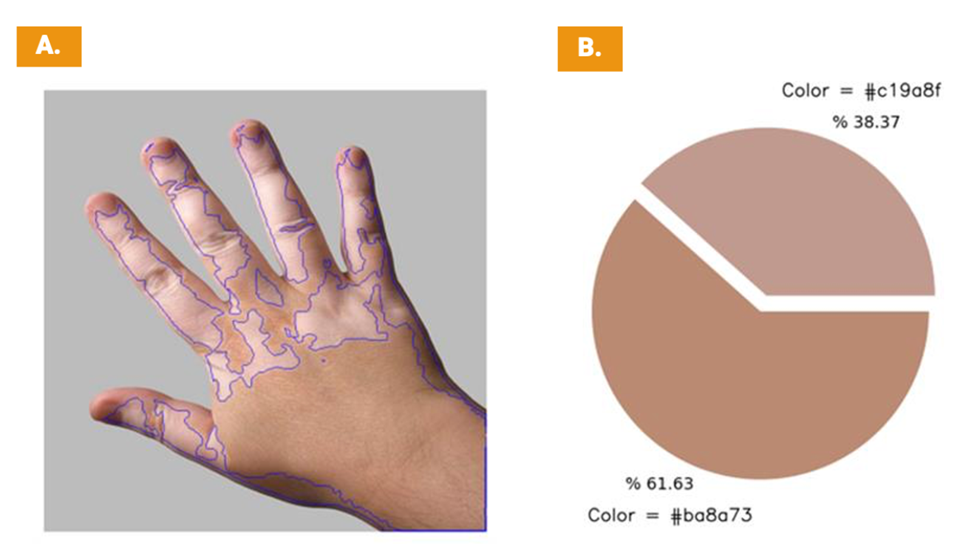
Figure 6. Segmentation and chromaticity output for mobile application users
Microbiome research: Studies have shown that fecal microbiota transplantation (FMT) can improve gut microbiota, increasing the repigmentation rate of phototherapy by 20%.
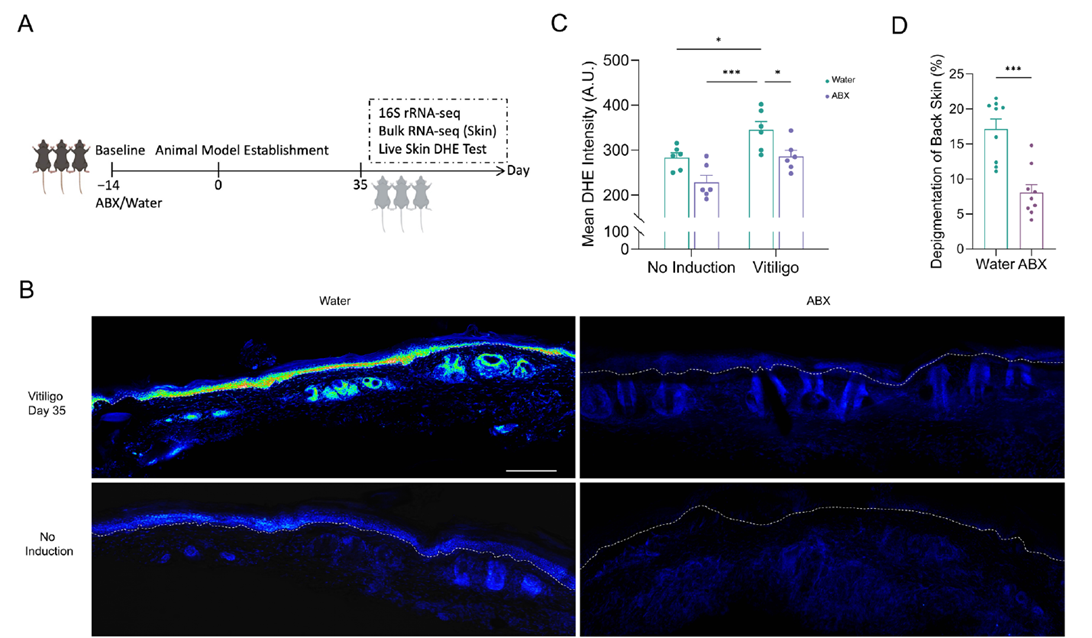
Figure 7. Gut microbiota is involved in vitiligo-related oxidative stress and melanocyte mitochondrial dysfunction in the skin
Biologics: AMG714 targeting IL-15 reduced TRM and stabilized disease progression in Phase II trials.
Stem cell therapy: Melanocyte stem cell transplantation combined with NB-UVB achieved an 80% repigmentation rate in patients with stable vitiligo.
Key Research Targets
JAK/STAT pathway: IFN-γ activates JAK1/2, leading to CXCL10 expression. Targets: JAK inhibitors such as ruxolitinib. Oral JAK inhibitor (tofacitinib) combined with NB-UVB achieved a 70% repigmentation rate at 6 months.
IFN-γ/CXCL9/10 axis: Recruits T cell infiltration via CXCR3. Targets: anti-IFN-γ monoclonal antibodies and CXCL10 blockers. Ritlecitinib (PF-06651600), a JAK3/TEC inhibitor, has shown preliminary efficacy in vitiligo clinical studies, though its primary approved indication is alopecia areata.
TRM and Treg cells: TRM maintains recurrence, while Treg cells suppress immunity. Targets: IL-15 inhibitors (e.g., AMG714) or CCR4 agonists to promote Treg migration. Studies have shown that NKG2D inhibitors targeting CD122 reduce TRM and prevent recurrence in animal models.
Oxidative stress pathway: NRF2 activation exerts antioxidant effects. Targets: NRF2 agonists such as dimethyl fumarate. Research analysis has shown that antioxidant supplementation (e.g., vitamin E) is effective as an adjuvant to phototherapy.
These targets are entering clinical trials with broad prospects, but attention should be paid to drug resistance and long-term safety.
abinScience Related Products
The following products from abinScience target core vitiligo research pathways, including the IFN-γ/CXCL9/10 axis, JAK/STAT signaling, IL-15/TRM biology, oxidative stress (NRF2), and melanocyte autoantigens (TYR). Catalog numbers link directly to the product pages.
Antibody
| Catalog No. |
Product Name |
| HF813016 |
Anti-Human IFN-gamma Reference Antibody (Emapalumab, RUO) |
| HF813026 |
Anti-Human IFN-gamma Reference Antibody (Fontolizumab, RUO) |
| HW541016 |
Anti-Human IL-15 Reference Antibody (Humax-IL15, RUO) |
| HW541036 |
Anti-Human IL-15 Reference Antibody (DISC0280, RUO) |
| HY524016 |
Anti-Human CXCL10/IP-10 Reference Antibody (Eldelumab, RUO) |
| HY524026 |
Anti-Human CXCL10/IP-10 Reference Antibody (NI-0801, RUO) |
Protein
| Catalog No. |
Product Name |
| HF813022 |
Recombinant Human IFNG/IFN-gamma Protein, N-His |
| HB829012 |
Recombinant Human JAK1 Protein, N-His |
| HT091012 |
Recombinant Human JAK2 Protein, N-His |
| HW746012 |
Recombinant Human STAT1 Protein, N-His |
| HW541012 |
Recombinant Human IL15 Protein, C-His |
| HB912011 |
Recombinant Human CD122/IL2RB Protein, C-His |
| HV388012 |
Recombinant Human FOXP3 Protein, N-His |
| HY029012 |
Recombinant Human HSPA1A Protein, N-His |
| HS810012 |
Recombinant Human NFE2L2/NRF2 Protein, N-His |
| HB200012 |
Recombinant Human TYR/Tyrosinase Protein, N-His |
| HB829022 |
Recombinant Human JAK1 Protein, C-His |
| HV388022 |
Recombinant Human FOXP3 Protein, N-His-SUMO |
| HF565012 |
Recombinant Human IFNA1/Interferon alpha-D Protein, N-His |
| HF879012 |
Recombinant Human TNFa/TNF-alpha Protein, N-His |
| HS856011 |
Recombinant Human IL17A Protein, C-His |
Show more Protein products
Looking for Vitiligo Research Tools?
abinScience provides factory-direct recombinant proteins and antibodies for IFN-γ, JAK/STAT, IL-15, CXCL10, NRF2, and TYR targets — with bulk pricing, custom specifications, and technical consultation available.
Email: info@abinscience.com | Tel: +86-27-65523339
References:
1. Ni Q, Xia L, Huang Y, et al. Gut microbiota dysbiosis orchestrates vitiligo-related oxidative stress through the metabolite hippuric acid. Microbiome. 2025;13(1):112. doi: 10.1186/s40168-025-02102-0
2. Chang WL, Ko CH. The Role of Oxidative Stress in Vitiligo: An Update on Its Pathogenesis and Therapeutic Implications. Cells. 2023;12(6):936. doi: 10.3390/cells12060936
3. Li W, Dong P, Zhang G, Hu J, Yang S. Emerging Therapeutic Innovations for Vitiligo Treatment. Curr Issues Mol Biol. 2025;47(3):191. doi: 10.3390/cimb47030191
4. Parikh M, Fang G, Poon F, et al. Technological advances in vitiligo management: perspectives on AI, mobile tools, and clinical utility. Front Med (Lausanne). 2025;12:1661554. doi: 10.3389/fmed.2025.1661554
5. Diotallevi F, Gioacchini H, De Simoni E, et al. Vitiligo, from Pathogenesis to Therapeutic Advances: State of the Art. Int J Mol Sci. 2023;24(5):4910. doi: 10.3390/ijms24054910
6. Seneschal J, Bae JM, Ezzedine K, et al. Vitiligo. Nat Rev Dis Primers. 2025;11:85. doi: 10.1038/s41572-025-00670-x
7. Speeckaert R, Caelenberg EV, Belpaire A, Speeckaert MM, Geel NV. Vitiligo: From Pathogenesis to Treatment. J Clin Med. 2024;13(17):5225. doi: 10.3390/jcm13175225

 中文
中文 English
English 한국어
한국어 日本語
日本語 Español
Español Français
Français Русский
Русский


