From June 5 to 8, 2026, the 86th American Diabetes Association (ADA) Scientific Sessions took place in New Orleans, USA. As the largest academic conference in the global field of diabetes and metabolic diseases, this year's annual meeting featured more than 20 symposia dedicated to obesity and energy metabolism, releasing the latest clinical data for over 30 drug candidates.
Multiple investigational anti-obesity agents in Phase II or Phase III clinical development were featured at the meeting, spanning various technological modalities such as single-target GLP-1 receptor agonists (RAs), dual-target (GLP-1/GIP, GLP-1/amylin, GCG/GLP-1) and triple-target (GLP-1/GIP/GCG) agonists, oral small-molecule GLP-1RAs, and ultra-long-acting injectables.

Figure 1. ADA Conference (Source: ADA)
1. Key Weight-Loss Drugs to Watch at ADA 2026
This year's meeting unveiled the latest clinical data for several weight-loss medications, covering diverse technological approaches from single- to triple-target mechanisms and from injectables to oral formulations. Overall, the data highlight a continuous upward trend in weight-loss efficacy and the accelerated maturation of oral formulations (see table below).
| Drug |
Company |
Target / Mechanism |
Key Clinical Data (ADA 2026) |
| LY3437943 |
Eli Lilly |
GLP-1/GIP/GCG triple receptor agonist |
TRIUMPH-1 Study: 28.3% weight loss in the 12 mg group at 80 weeks; up to 30.3% weight loss in the 104-week extension; 16.8% weight loss at 40 weeks in the type 2 diabetes (T2D) subgroup, with approximately 90% of patients achieving HbA1c < 7%. |
| LY3502970 |
Eli Lilly |
Oral small-molecule GLP-1 receptor agonist (non-peptide) |
ATTAIN-1 Study: 12.4 kg (12.4%) weight loss in the highest dose group, showing head-to-head superiority over oral semaglutide; no pre-meal fasting required. |
| CagriSema |
Novo Nordisk |
Semaglutide + cagrilintide (amylin analogue) fixed-dose combination |
REIMAGINE Phase III Series: 13.8% weight loss in the high-dose group at 40 weeks, with a 1.8 percentage point reduction in HbA1c; fMRI demonstrated altered activity in appetite-related brain regions, including the dorsomedial thalamus and putamen. |
| Zenagamtide |
Novo Nordisk |
GLP-1/amylin dual-receptor unimolecular agonist |
Phase II Trial (36 weeks): 14.6% weight loss in the 40 mg group alongside significant reductions in HbA1c; gastrointestinal adverse events were predominantly mild-to-moderate. |
| Ecnoglutide |
Sciwind Biosciences/Pfizer |
GLP-1 receptor agonist |
SLIMMER-UP-SWITCH Phase II Head-to-Head Study (20 weeks): 12.8% weight loss, representing a 35% improvement over semaglutide; achieved a ≥10% weight loss responder rate of 74.4%. |
| IBI362 |
Innovent Biologics |
GCG/GLP-1 dual receptor agonist |
GLORY-2 Study (60 weeks): 18.55% weight loss in the 9 mg group, with 44% of patients achieving ≥20% weight loss; demonstrated head-to-head superiority over semaglutide. |
| Elecoglipron |
Eccogene/AstraZeneca |
Oral small-molecule GLP-1 receptor agonist |
VISTA Study (36 weeks): 11.8% weight loss in the 75 mg group, with no plateau observed on the weight-loss curve; Phase IIb results published in The Lancet. |
| Berobenatide |
Pfizer (acquired Metsera) |
Ultra-long-acting GLP-1 receptor agonist (once monthly) |
Phase IIb Extension Study: Once-monthly dosing achieved an initial weight loss of 12.3% (with weight continuing to decrease at data cutoff). |
| ASC30 |
Ascletis Pharma |
Oral small-molecule fully biased GLP-1R agonist |
Phase II (13 weeks): Dose-dependent weight loss with no plateau observed; favorable gastrointestinal tolerability, with lower incidence rates of nausea and vomiting compared to similar oral drugs. |
| RAY1225 |
Rays Pharma |
GLP-1/GIP dual receptor agonist |
Phase II (24 weeks): 21.18% weight loss in the 18 mg group, with 100% of participants achieving >15% weight reduction. |
| Repupotide |
Hengrui Medicine |
GLP-1/GIP dual receptor agonist |
Oral formulation Phase II (26 weeks) showed continuous weight loss; injectable formulation Phase III completed, with the New Drug Application (NDA) accepted by the NMPA. |
As illustrated in the table, despite the distinct mechanisms of action among these candidate drugs, a clear paradigm emerges: targeting more receptors correlates with greater weight loss. Single-target GLP-1R agonists yield a maximum weight reduction of approximately 12–15%, dual-target agents typically achieve 18–21%, and the triple-target agonist LY3437943 has breached the 30% threshold. Underlying this trend is a deepening scientific understanding of the human energy metabolism regulatory network.
2. From Single-Target to Multi-Target: The Underlying Logic of Mechanistic Evolution
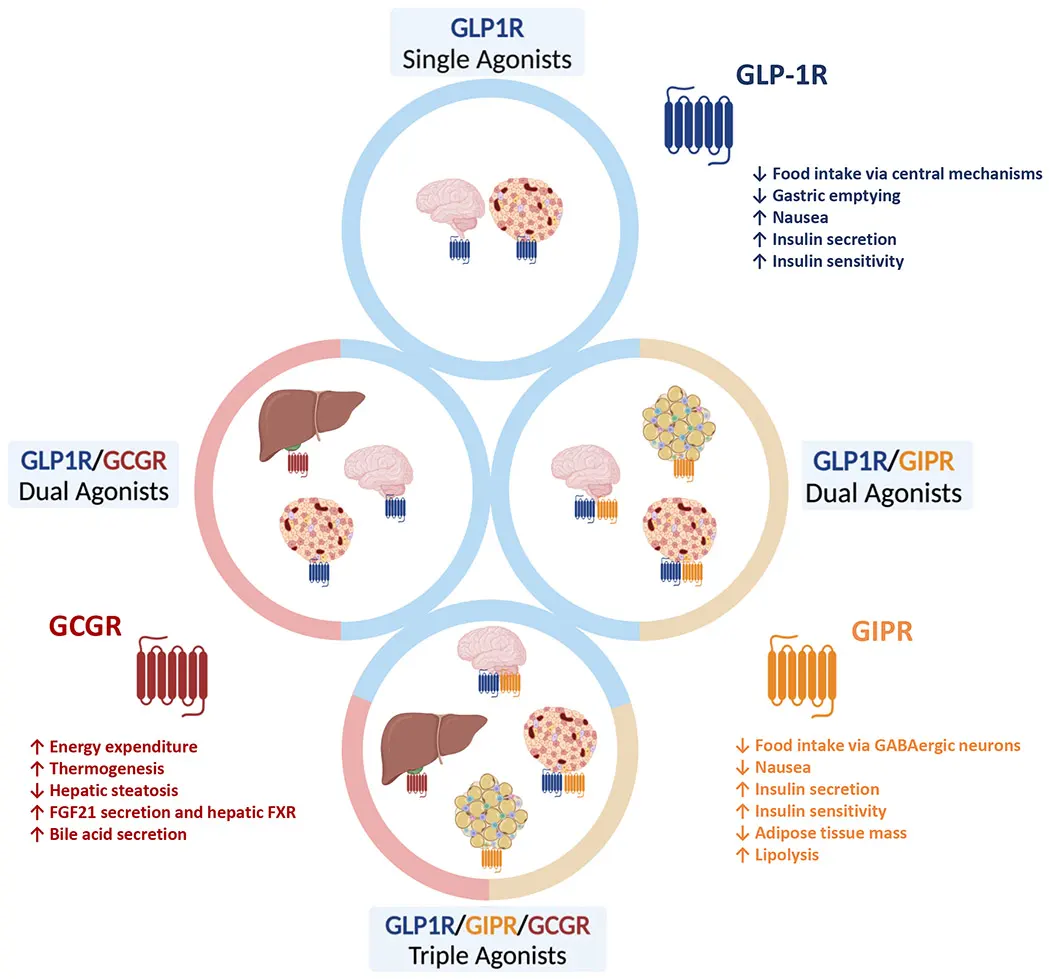
Figure 2. Main sites of action and tissue-specific effects of different agonists (Source: DOI: 10.1016/j.cell.2024.06.003)
The rise of GLP-1 receptor agonists represents one of the most significant breakthroughs in the treatment of metabolic diseases over the past decade. By activating the GLP-1 receptor, these agents stimulate insulin secretion, suppress appetite, and delay gastric emptying, thereby delivering profound glucose-lowering and weight-reducing efficacy. However, as clinical data have accumulated, researchers have increasingly recognized a bottleneck: single-target GLP-1R agonists hit a therapeutic plateau for weight loss at around 12–15%, leaving limited room for further improvement.
This bottleneck has prompted investigators to re-evaluate the regulatory networks governing human energy metabolism. In reality, body weight maintenance does not rely on a single signaling pathway; rather, it is tightly regulated by multiple interconnected hormonal axes involving the coordinated interplay of various organs, including the gut, pancreas, adipose tissue, and brain. Consequently, an increasing number of studies are exploring the simultaneous activation of multiple metabolic pathways to achieve deeper metabolic regulation. Based on data from this year's conference, the most prominent multi-target combinations include:
- • GLP-1R + GIPR (Dual-Target): Synergistically enhances satiety and remodels lipid metabolism.
- • GLP-1R + GCGR (Dual-Target): Escalates basal energy expenditure while maintaining glycemic control.
- • GLP-1R + Amylin Receptor (Dual-Target): Amplifies appetite suppression through dual peripheral and central pathways.
- • GLP-1R + GIPR + GCGR (Triple-Target): Drives multi-dimensional synergy, pushing weight loss beyond the 28–30% threshold.
Comprehending why these combinations are effective requires a deep dive into the biological foundations and drug design rationale of each specific target.
3. Biological Foundations and Drug Design Rationale of Key Targets
3.1 GLP-1 Receptor (GLP-1R) — The Cornerstone of Multi-Target Therapeutics
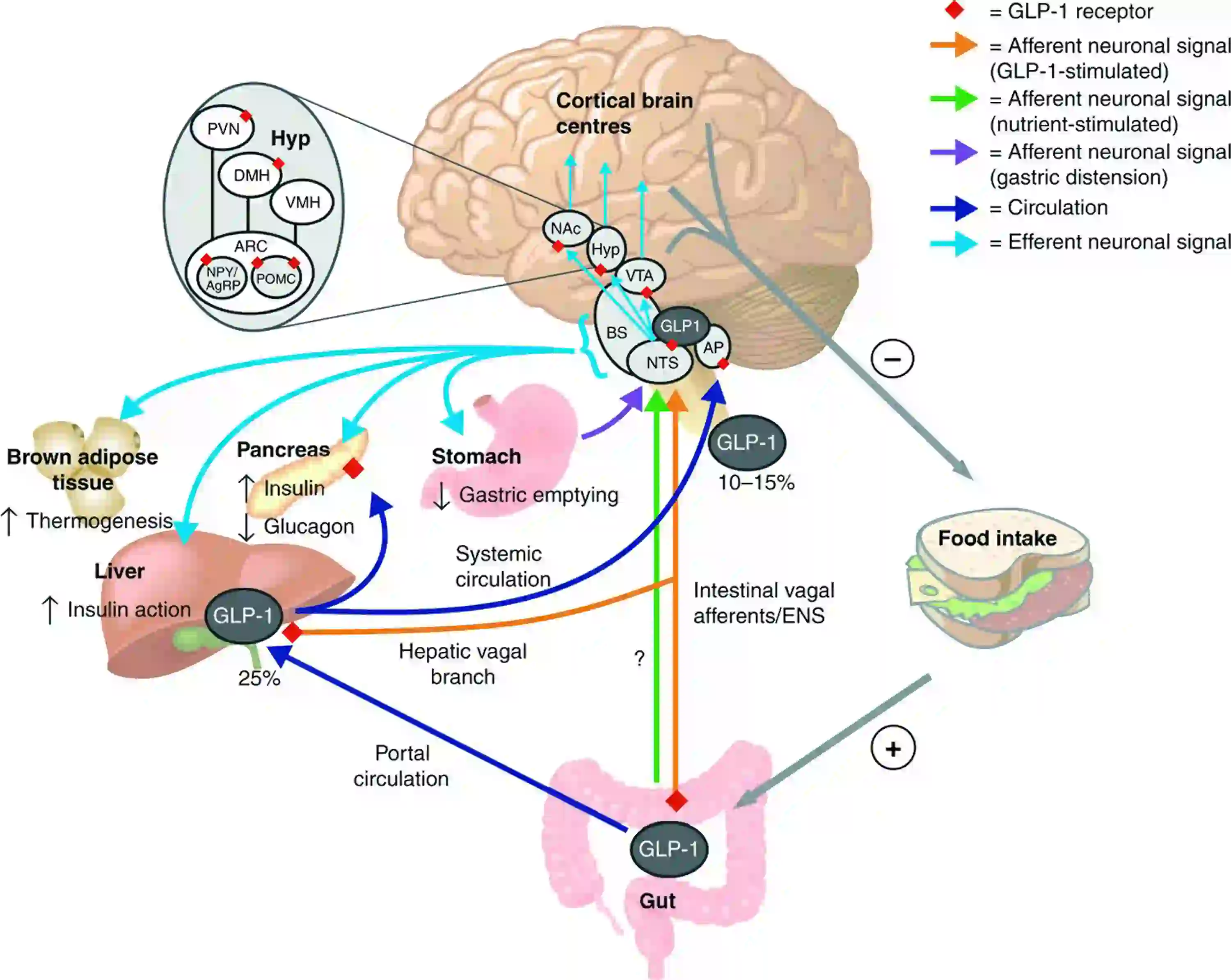
Figure 3. Schematic mechanism of GLP-1 in the central regulation of food intake and glucose metabolism(Source: DOI: 10.1016/j.amjmed.2025.01.021)
GLP-1R is a class B G-protein coupled receptor (GPCR) widely distributed across pancreatic β-cells, the gastrointestinal tract, vagal ganglia, and the hypothalamus. Its native ligand, GLP-1, is secreted by intestinal L-cells postprandially and exerts its physiological functions by activating GLP-1R, which include glucose-dependent insulin secretion, inhibition of glucagon release, delayed gastric emptying, and direct appetite suppression via action on the arcuate nucleus of the hypothalamus.
At this year's meeting, whether dealing with single-target agents (e.g., ecnoglutide, LY3502970, berobenatide) or multi-target agents (e.g., LY3437943, CagriSema, IBI362), GLP-1R activation was universally retained. This underscores that GLP-1R agonism remains the foundational prerequisite for current weight-loss drug design, with additional targets serving as "add-on synergistic enhancers".
Nevertheless, because the efficacy ceiling for single-target GLP-1R agonism plateaus at ~12–15%, breaching this threshold necessitates incorporating secondary targets that offer complementary regulatory dimensions.
3.2 GIP Receptor (GIPR) — A Synergistic Target for Enhanced Weight-Loss Efficacy
GIPR is also a class B GPCR, abundantly expressed in pancreatic β-cells, adipose tissue, bone, and the central nervous system (CNS). Its native ligand, GIP, is secreted by intestinal K-cells following nutrient ingestion. While early literature suggested that GIP might promote obesity, recent insights have revealed that in the presence of GLP-1R co-activation, GIPR agonism markedly amplifies GLP-1-mediated weight loss. The proposed mechanisms involve modulating lipid storage and metabolism in adipose tissue, as well as synergizing within the CNS to enhance satiety.
Data presented at this ADA meeting for the GLP-1/GIP dual agonist RAY1225 (21.18% weight loss) and the triple agonist LY3437943 (28–30% weight loss) strongly validate this synergistic effect. Notably, the structural design of GIPR agonists must carefully consider biased signaling; prioritizing the cAMP pathway over β-arrestin recruitment helps minimize receptor desensitization and optimizes long-term therapeutic durability.
While the inclusion of GIPR focuses primarily on "efficacy enhancement," the integration of GCGR addresses an entirely different dimension: increasing basal energy expenditure.
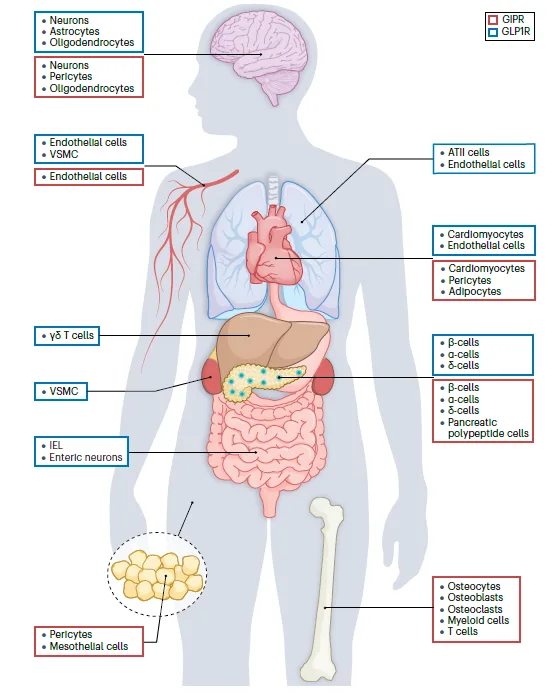
Figure 4. Tissue-specific expression of GLP-1R and GIPR(Source: DOI: 10.1038/s41574-022-00783-3)
3.3 Glucagon Receptor (GCGR) — A Regulatory Target for Basal Energy Expenditure
GCGR is predominantly expressed in the liver, kidneys, and adipose tissue. Its native ligand, glucagon, is secreted by pancreatic α-cells during hypoglycemia to stimulate glycogenolysis, gluconeogenesis, and fatty acid oxidation, thereby increasing total body energy expenditure. Because standalone GCGR agonists induce hyperglycemia, they cannot be used in isolation for obesity management. However, when co-formulated with a GLP-1R agonist, GCGR activation counteracts the reduction in metabolic rate typically triggered by GLP-1, producing a robust synergistic effect of glucose lowering and increased energy expenditure.
Data from this conference demonstrated that IBI362 (GCG/GLP-1 dual agonist) achieved 18.55% weight loss, while LY3437943 (GLP-1/GIP/GCG triple agonist) reached up to 30% weight loss. This underscores that the recruitment of GCGR is a pivotal factor in unlocking profound weight reduction (>25%). Concurrently, investigators must monitor potential risks of elevated heart rate and blood pressure associated with GCGR agonism; however, safety profiles from LY3437943 indicate that these risks remain generally manageable.
While GCGR targets peripheral metabolism, the amylin receptor discussed below acts at the peripheral-CNS interface—specifically the area postrema—providing a complementary dimension by regulating postprandial satiety signals.
3.4 Amylin Receptor — A Central Satiety Signaling Target
The amylin receptor is a heterodimeric complex composed of a calcitonin receptor (CTR) core and receptor activity-modifying proteins (RAMPs), belonging to the class B GPCR family. Its native ligand, amylin, is co-secreted with insulin by pancreatic β-cells. Its physiological actions include delaying gastric emptying, suppressing postprandial glucagon secretion, and acting on the area postrema of the brainstem to generate potent satiety signals.
Amylin and GLP-1 exhibit synergistic effects on appetite suppression and gastric emptying without compounding adverse events. At this meeting, both CagriSema (a semaglutide + cagrilintide fixed-dose combination) and Zenagamtide (a unimolecular GLP-1/amylin dual agonist) validated this synergy. Of particular note, the fMRI data for CagriSema provided the first direct confirmation of the drug's capacity to modulate neural activity within appetite-regulating brain regions, such as the dorsomedial thalamus and the putamen, offering objective radiographic evidence for mechanistic research.
The aforementioned four receptor classes are peptide receptors, and therapeutics targeting them have traditionally been dominated by injectable modalities. However, another standout highlight of this conference was the comprehensive maturation of oral small-molecule GLP-1R agonists. These small molecules feature distinct binding pockets compared to peptides, carving out differentiated design opportunities.
3.5 Oral Small-Molecule GLP-1R Agonists — Transmembrane Binding and Biased Activation Strategies
Unlike peptide GLP-1R agonists that interact with the receptor's extracellular domain, oral small-molecule agonists (such as LY3502970, elecoglipron, and ASC30) typically bind within the transmembrane domain. This structural divergence yields two profound advantages: first, their low molecular weight significantly enhances oral bioavailability; second, they can be strategically engineered as biased agonists that selectively couple with G-protein signaling pathways while avoiding β-arrestin recruitment. This minimizes receptor internalization and desensitization, prolongs the duration of action, and potentially mitigates the incidence of gastrointestinal adverse effects.
Phase II data for ASC30 (a fully biased GLP-1R agonist) were particularly striking at this conference: while delivering robust weight loss, its incidence of nausea and vomiting was significantly lower than that of contemporary oral GLP-1 candidates, charting a new path for optimizing tolerability. Additionally, the ATTAIN-1 study for LY3502970 demonstrated head-to-head superiority over existing oral semaglutide without requiring pre-meal fasting, vastly improving patient convenience.
4. Industry and Technological Trends
Synthesizing the clinical data and mechanistic insights from this year's ADA meeting, four prominent technological trends are shaping the future landscape of anti-obesity therapeutics.
Trend 1: Multi-target synergy as the core strategy for maximizing efficacy.
The progression of weight-loss percentages from 12–15% (single-target) to 18–22% (dual-target) and ultimately 28–30% (triple-target) reflects systemic intervention across multiple nodes of the energy metabolism network. Different target combinations yield distinct mechanistic advantages: GIPR-containing agents rely heavily on adipose tissue remodeling and CNS synergy; GCGR-containing candidates prioritize elevating basal energy expenditure; while amylin-receptor-containing agents demonstrate superior postprandial glucose control and central satiety signaling. Future paradigms may witness customized target combinations tailored to individual metabolic phenotypes.
Trend 2: Oral small-molecule GLP-1R agonists hitting maturity.
The confirmatory clinical datasets released at this meeting for multiple oral, non-peptide GLP-1R agonists prove that this technological route has transitioned from niche exploration into mainstream drug development. Compared to injectable formulations, oral small molecules offer unparalleled compliance advantages across large patient populations. Future development directions include ultra-long-acting oral formulations (to reduce dosing frequency), biased activation architectures to enhance gastrointestinal tolerance (such as ASC30), and dosage optimization tailored for specific cohorts like elderly or renally impaired patients.
Trend 3: Ultra-long-acting formulations reshaping dosing paradigms.
The Phase IIb data for once-monthly berobenatide represents a seminal attempt toward minimizing dosing frequency. For chronic metabolic diseases requiring lifelong management, reducing injection frequency dramatically enhances long-term patient adherence. Critical challenges to address moving forward include evaluating the risk of systemic accumulation, understanding the latency of efficacy decay post-discontinuation, and devising personalized dose-titration strategies.
Trend 4: Neuroimaging methodologies deepening mechanistic research.
The fMRI data unveiled in the CagriSema studies visually map out drug-induced alterations in neural activity within appetite-regulating brain structures, offering a novel, objective endpoint for decoding the central mechanisms of anti-obesity therapeutics. This methodological advance holds promise for predicting individual patient response, guiding early-stage target screening, and optimizing dosing regimens, making it a highly valuable tool in the clinical development pipeline.
Conclusion
This year's ADA Scientific Sessions highlighted several high-caliber clinical studies in the obesity space, spanning single- to triple-target pathways, injectables to oral formulations, and weekly to monthly schedules. Functioning as the core therapeutic anchor, GLP-1R co-activation with GIPR, GCGR, or the amylin receptor has pushed achievable weight loss from the historical 12–15% baseline to over 30%. Clinically validated oral small-molecule GLP-1R agonists, through biased signaling designs, offer compelling pathways to optimize patient tolerability. Furthermore, the deployment of ultra-long-acting modalities and neuroimaging tools is expanding the frontiers of clinical development and mechanistic discovery in metabolic disease.
These advances expand the therapeutic armamentarium for obesity and related metabolic disorders (including type 2 diabetes, non-alcoholic steatohepatitis (NASH), and obstructive sleep apnea), while also raising key scientific questions for basic research: the optimal ratio of target engagement and personalized indications for different combination regimens, mechanisms of metabolic adaptation and weight rebound after long-term administration, and optimal strategies for combining pharmacotherapy with non-pharmacological interventions — all of which require further investigation.
For a detailed comparison of PK ELISA kits, ADA screening assays, and receptor antibodies across semaglutide, tirzepatide, and LY3437943 — including product specs, validation data, and assay design guidance — see our Incretin Drug Research Reagent Comparison Guide.
abinScience closely follows cutting-edge research in obesity and metabolic disease drug development, providing high-quality protein and antibody products for key weight-loss targets. To meet the research needs of the broader research community for key receptors including GLP-1, GIP, GCGR, and amylin, our company has developed a series of high-activity recombinant proteins, highly specific antibodies, and related assay kits. Click on the catalog number to access product details directly.
| Product Type |
Catalog No. |
Product Name |
| Protein |
HP899012 |
Recombinant Tirzepatide Protein, N-GST & C-His |
| HY040012 |
Recombinant Human GIP Protein, N-His |
| HT451012 |
Recombinant Human GIPC1 Protein, N-His |
| HF737012 |
Recombinant Human GCG Protein, N-His |
| HW595012 |
Recombinant Human GIPR/GIP-R Protein, N-His |
| Antibody |
SW328046 |
Research Grade LY3437943 |
| SW328036 |
Research Grade LY3502970 |
| YD684014 |
Anti-IBI362 Polyclonal Antibody |
| HW328024 |
Anti-LY3437943 Polyclonal Antibody |
| HP899014 |
Anti-Semaglutide (GLP-1 analogue) Polyclonal Antibody |
| HW328036 |
Anti-Human GLP-1R Reference Antibody (mAb-36986, RUO) |
| HW328016 |
Anti-Human GLP-1R Reference Antibody (GMA105, RUO) |
| HW595026 |
Anti-Human GIPR&GLP-1R Reference Antibody (AMG 133, RUO) |
| HF737016 |
Research Grade Efpegerglucagon |
| HW328026 |
Research Grade Gulgafafusp Alfa |
| HW595016 |
Anti-Human GIPR Reference Antibody (Maridebart, RUO) |
| HY040013 |
Anti-Human GIP Recombinant Antibody (SAA1567) |
| MW595010 |
InVivoMAb Anti-Mouse GIPR Antibody (Iv0037) |
| HW595013 |
Anti-Human GIPR/GIP-R Recombinant Antibody (SAA1449) |
| HW547016 |
Anti-Human Glucagon R/GCGR Reference Antibody (Volagidemab, RUO) |
| HW547026 |
Anti-Human Glucagon R/GCGR Reference Antibody (Crotedumab, RUO) |
| Kit |
AW328018 |
Anti-LY3437943 Human IgG ELISA Kit |
| DW328058 |
LY3437943 ELISA Kit |
| DW328048 |
LY3502970 ELISA Kit |
| DD684018 |
IBI362 ELISA Kit |
| AD684018 |
Anti-IBI362 ELISA Kit |
References
- [1] Holst J. J. (2024). GLP-1 physiology in obesity and development of incretin-based drugs for chronic weight management. Nature metabolism, 6(10), 1866–1885. https://doi.org/10.1038/s42255-024-01113-9
- [2] Hammoud, R., & Drucker, D. J. (2023). Beyond the pancreas: contrasting cardiometabolic actions of GIP and GLP1. Nature reviews. Endocrinology, 19(4), 201–216. https://doi.org/10.1038/s41574-022-00783-3
- [3] Del Prato S, Gallwitz B, Holst JJ, Meier JJ. The incretin/glucagon system as a target for pharmacotherapy of obesity. Obes Rev. 2022 Feb;23(2):e13372. doi: 10.1111/obr.13372. Epub 2021 Oct 28. PMID: 34713962; PMCID: PMC9286339.
- [4]Beutler L. R. (2026). GLP-1 physiology and pharmacology along the gut-brain axis. The Journal of clinical investigation, 136(2), e194744. https://doi.org/10.1172/JCI194744
- [5] Bajaj, H. S., Welch, M., Shah, P., Luna, E., Jaouimaa, F. Z., Liu, B., Liu, R., Chen, Y., Patel, H., & Bartee, A. (2026). Efficacy and safety of LY3437943, a GIP, GLP-1, and glucagon receptor agonist, in people with type 2 diabetes and inadequate glycaemic control with diet and exercise (TRANSCEND-T2D-1): a double-blind, randomised, phase 3 trial. Lancet (London, England), S0140-6736(26)00967-0. Advance online publication. https://doi.org/10.1016/S0140-6736(26)00967-0
- [6] Kusminski, C. M., Perez-Tilve, D., Müller, T. D., DiMarchi, R. D., Tschöp, M. H., & Scherer, P. E. (2024). Transforming obesity: The advancement of multi-receptor drugs. Cell, 187(15), 3829–3853. https://doi.org/10.1016/j.cell.2024.06.003
- [7] Moiz, A., Filion, K. B., Tsoukas, M. A., Yu, O. H., Peters, T. M., & Eisenberg, M. J. (2025). Mechanisms of GLP-1 Receptor Agonist-Induced Weight Loss: A Review of Central and Peripheral Pathways in Appetite and Energy Regulation. The American journal of medicine, 138(6), 934–940. https://doi.org/10.1016/j.amjmed.2025.01.021
- [8] Wang, S., Liu, Y., Yan, Z., Huang, X., Liao, Y., Tang, C., Jing, L., Zhou, Z., Han, J., Tang, W., & Jiang, N. (2025). Strategic Design of Triple GLP-1R/GCGR/GIPR Agonists with Varied Receptor Potency: Achieving Comparable Glycemic and Weight Reduction Effects. Journal of medicinal chemistry, 68(19), 20765–20788. https://doi.org/10.1021/acs.jmedchem.5c02032
- [9] Araki, E., Sakaguchi, M., Fukuda, K., & Kondo, T. (2022). Potential of a glucagon-like peptide-1 receptor/glucose-dependent insulinotropic polypeptide receptor/glucagon receptor triagonist for the treatment of obesity and type 2 diabetes. Journal of diabetes investigation, 13(12), 1958–1960. https://doi.org/10.1111/jdi.1389

 中文
中文 English
English 한국어
한국어 日本語
日本語 Español
Español Français
Français Русский
Русский


