2026 Breast Cancer Research Review: Molecular Subtypes, ADC Breakthroughs & Research Reagents
Release date:
2026-05-13 View count: 123
2026 Breast Cancer Research Review: Molecular Subtypes, ADC Breakthroughs & Research Reagents
Two years ago, roughly half of all metastatic breast cancer patients were handed a diagnosis of "HER2-negative" and steered toward conventional chemotherapy. That category no longer exists in the same form. The approval of trastuzumab deruxtecan (T-DXd) for HER2-low disease — and the emerging data extending its benefit to HER2-ultralow tumors — has redrawn the treatment map for the world's most common malignancy (~2.3 million new cases per year). In parallel, TROP-2-targeted ADCs are reshaping triple-negative breast cancer (TNBC) management, while CDK4/6 inhibitors and next-generation endocrine agents continue to extend survival for hormone receptor-positive patients. This review examines the molecular logic behind these shifts and maps them to the research reagents needed to study, validate, and develop the next generation of therapies.
Four Diseases Under One Name: Breast Cancer Molecular Subtypes
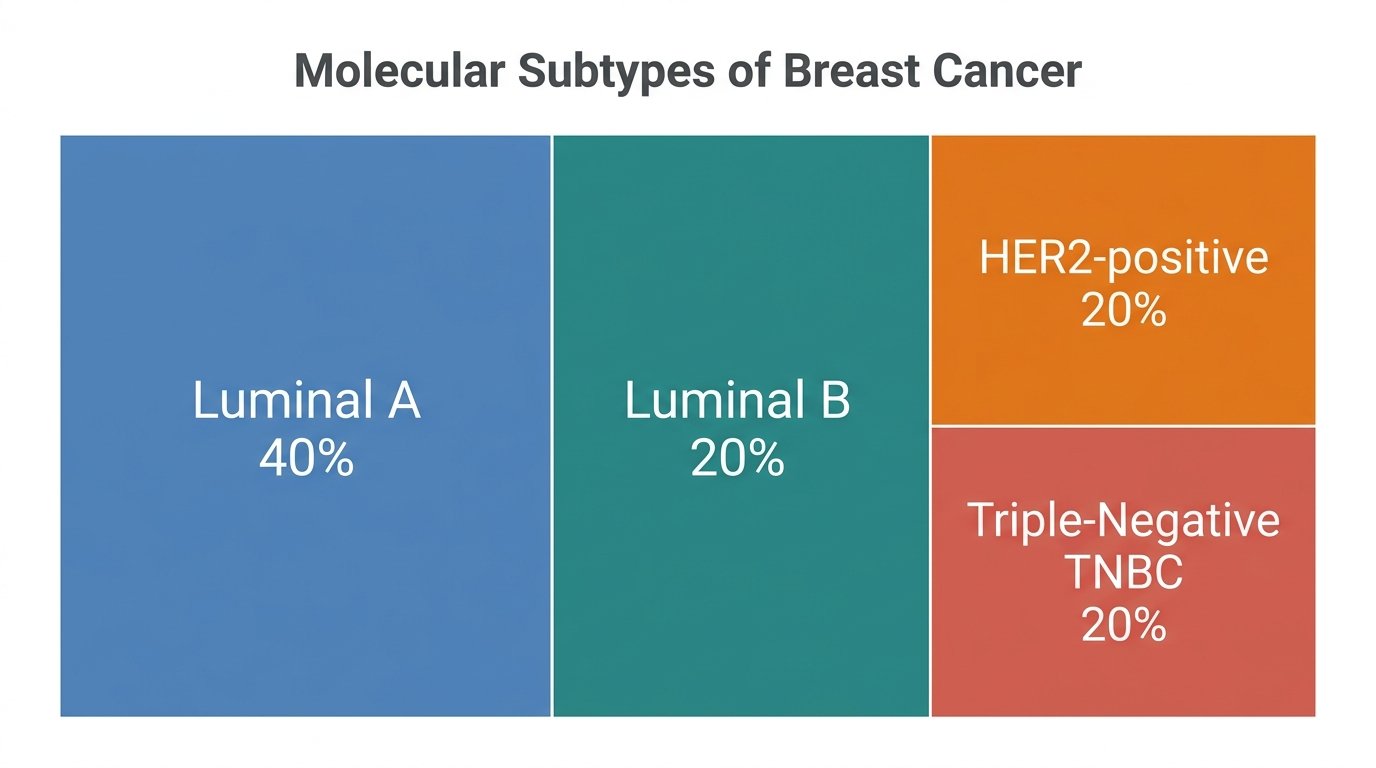
Breast cancer is not a single disease. Molecular profiling has resolved it into at least four subtypes with distinct biology, distinct prognosis, and — critically — distinct druggable targets. Understanding which subtype a tumor belongs to now determines the entire treatment sequence from neoadjuvant to metastatic setting.
Figure 1. Molecular Subtypes of Breast Cancer. Luminal A (~40%), Luminal B (~20%), HER2-positive (~20%), and Triple-Negative TNBC (~20%).
Subtype
Defining Features
Frequency
Druggable Biology
Current Treatment Backbone
Luminal A
ER+/PR+, HER2−, low Ki-67
~40%
Estrogen-driven proliferation via ER/ESR1; cyclin D1–CDK4/6 cell cycle control; PIK3CA hotspot mutations in ~40% of cases
Endocrine therapy ± CDK4/6 inhibitor (palbociclib, ribociclib, abemaciclib); alpelisib for PIK3CA-mutant; capivasertib for AKT-pathway altered
Luminal B
ER+/PR±, HER2±, high Ki-67
~20%
Higher proliferative index with earlier endocrine resistance; acquired ESR1 mutations drive ligand-independent ER activation in metastatic setting
Endocrine + CDK4/6 inhibitor; elacestrant (oral SERD for ESR1-mutant); T-DXd after endocrine failure if HER2-low/ultralow
Why It Matters for Reagent Selection: Each subtype requires a different set of research tools — ER/PR antibodies and CDK4/6 proteins for Luminal biology, HER2/HER3 recombinant proteins and biosimilar references for ADC development, TROP-2 antibodies and sacituzumab ELISA kits for TNBC drug screening, and BRCA1/2 proteins for DNA repair pathway studies.
From Binary to Spectrum: How T-DXd Redefined HER2
The story of HER2-low is fundamentally a story about drug design outrunning diagnostic categories.
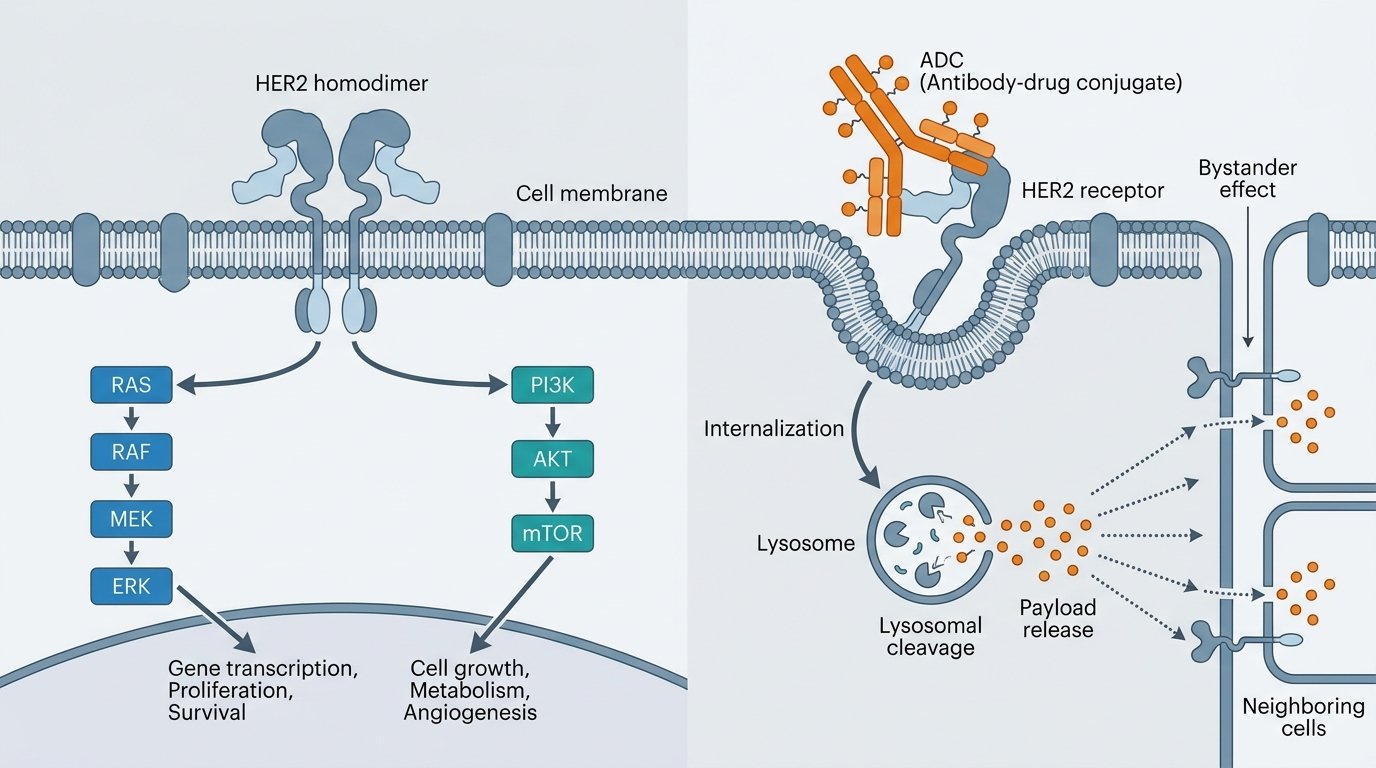
For two decades, HER2 status was binary: amplified (IHC 3+ or ISH+) or not. Patients scoring IHC 1+ or 2+/ISH− were grouped with IHC 0 as "HER2-negative" — a label that implied HER2-directed therapy was irrelevant. Trastuzumab deruxtecan changed this logic. Unlike earlier HER2-targeted agents, T-DXd combines a high drug-to-antibody ratio (DAR 8:1), a membrane-permeable topoisomerase I payload, and a cleavable linker that enables a bystander effect — killing neighboring tumor cells even if they express little or no HER2.
Figure 2. HER2 Signaling and ADC Mechanism of Action. Left: HER2 homodimerization drives RAS–MAPK and PI3K–AKT–mTOR cascades promoting proliferation and survival. Right: ADC binds surface HER2, undergoes receptor-mediated internalization, lysosomal linker cleavage releases the cytotoxic payload intracellularly; released payload diffuses to neighboring cells (bystander effect).
The clinical evidence that built this new category:
DESTINY-Breast04 (2022): T-DXd vs. chemotherapy in previously treated HER2-low (IHC 1+ or 2+/ISH−) metastatic breast cancer. Median PFS 9.9 vs. 5.1 months (HR 0.50); median OS 23.4 vs. 16.8 months (HR 0.64). This single trial created the "HER2-low" treatment category, reclassifying ~55% of previously "HER2-negative" patients as candidates for HER2-directed therapy [1].
DESTINY-Breast06 (2024): Extended the concept further — T-DXd vs. chemotherapy after endocrine therapy failure in HR+/HER2-low and HER2-ultralow (IHC 0 with any membrane staining). Median PFS 13.2 vs. 8.1 months (HR 0.62) in HER2-low, with consistent benefit in the ultralow subgroup. This positions T-DXd before chemotherapy in the treatment sequence [2].
The practical consequence: ASCO/CAP guidelines now require pathologists to report specific IHC scores (0, 1+, 2+, 3+) rather than simple positive/negative, because each score level now carries distinct therapeutic implications. Research-grade HER2 proteins across the full expression spectrum — and anti-drug antibody reagents for T-DXd PK/immunogenicity assays — are now essential components of any breast cancer translational research program.
The ADC Revolution & Immunotherapy: Clinical Milestones (2022–2026)
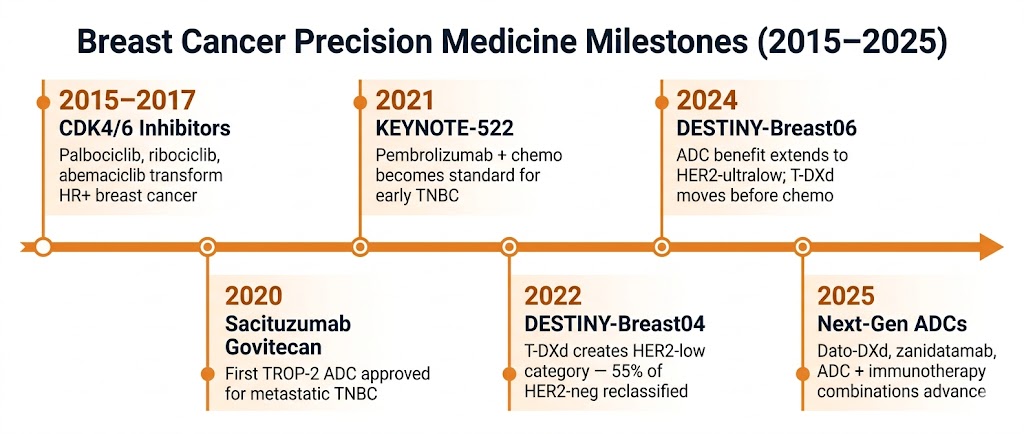
Figure 3. Breast Cancer Precision Medicine Milestones (2015–2025). From CDK4/6 inhibitors transforming HR+ disease, through TROP-2 ADCs and checkpoint immunotherapy in TNBC, to T-DXd redefining HER2-low and HER2-ultralow as treatable categories.
Trial & Agent
What It Showed
Why It Matters
Reference
DESTINY-Breast04
T-DXd in HER2-low mBC
PFS 9.9 vs. 5.1 mo (HR 0.50); OS 23.4 vs. 16.8 mo (HR 0.64) over chemotherapy. Benefit consistent in both HR+ and HR− cohorts.
Created HER2-low as a treatment category; first HER2-directed therapy for ~55% of previously "HER2-negative" patients.
[1]
DESTINY-Breast06
T-DXd in HER2-low/ultralow after ET
PFS 13.2 vs. 8.1 mo (HR 0.62) in HER2-low; consistent benefit in HER2-ultralow (IHC 0 with membrane staining).
Moves T-DXd before chemotherapy in HR+/HER2-low sequence; extends ADC reach to ultralow HER2 expression.
[2]
KEYNOTE-522
Pembrolizumab in early TNBC
pCR 64.8% vs. 51.2%; EFS HR 0.63; 5-year OS 86.6% vs. 81.7% (HR 0.66). 34% reduction in risk of death.
Established perioperative immunotherapy as standard of care for high-risk early TNBC — the first regimen to improve OS in this setting.
[3][4]
ASCENT
Sacituzumab govitecan in mTNBC
PFS 5.6 vs. 1.7 mo (HR 0.41); OS 12.1 vs. 6.7 mo (HR 0.48) over chemotherapy in pretreated metastatic TNBC.
Validated TROP-2 as a therapeutic target; first ADC to demonstrate survival benefit in metastatic TNBC.
[5]
monarchE
Adjuvant abemaciclib in HR+
5-year iDFS 83.6% vs. 76.0% (HR 0.68) with abemaciclib + endocrine therapy in high-risk HR+/HER2− early BC.
First and only CDK4/6 inhibitor with adjuvant benefit; now standard of care for high-risk HR+ early breast cancer.
[6]
CAPItello-291
Capivasertib in HR+ mBC
PFS 7.2 vs. 3.6 mo (HR 0.60); benefit enriched in PIK3CA/AKT1/PTEN-altered tumors (HR 0.50).
Adds a targeted option for endocrine-resistant HR+ disease; biomarker selection identifies the best responders.
[7]
What’s Next: ADCs are converging with immunotherapy — trials combining T-DXd or sacituzumab with checkpoint inhibitors are in Phase 2/3. Bispecific antibodies targeting HER2×HER3 (zanidatamab) and next-generation TROP-2 ADCs (datopotamab deruxtecan) are advancing rapidly. Research-grade biosimilars of these agents and companion PK/ADA assay reagents are critical for translational programs.
abinScience Breast Cancer Research Toolkit
The following product quick-reference tables are organized by research application. Each section can be expanded to view representative products with direct catalog links. For the complete listing of 600+ breast cancer reagents, use the search page linked below.
Showing 13 representative products across 7 target families. Full catalog includes 600+ breast cancer-related reagents.
abinScience — Empowering Bioscience Discovery 600+ breast cancer reagents spanning the full HER2 expression spectrum, TROP-2 ADC development tools, PD-1/PD-L1 checkpoint references, and hormone receptor pathway proteins. From target validation to PK/ADA assay development — one supplier, one quality standard.
Need help selecting the right reagent for your breast cancer project? Contact us: info@abinscience.com | Phone: +86-27-65523339
Modi S, Jacot W, Yamashita T, et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. 2022;387(1):9–20. doi:10.1056/NEJMoa2203690
Bardia A, Hu X, Dent R, et al. Trastuzumab deruxtecan after endocrine therapy in metastatic breast cancer. N Engl J Med. 2024;391(22):2110–2122. doi:10.1056/NEJMoa2407086
Schmid P, Cortes J, Dent R, et al. Event-free survival with pembrolizumab in early triple-negative breast cancer. N Engl J Med. 2022;386(6):556–567. doi:10.1056/NEJMoa2112651
Schmid P, Cortes J, Dent R, et al. Overall survival with pembrolizumab in early-stage triple-negative breast cancer. N Engl J Med. 2024;391(21):2003–2014. doi:10.1056/NEJMoa2409932
Bardia A, Hurvitz SA, Tolaney SM, et al. Sacituzumab govitecan in metastatic triple-negative breast cancer. N Engl J Med. 2021;384(16):1529–1541. doi:10.1056/NEJMoa2028485
Johnston SRD, Harbeck N, Hegg R, et al. Abemaciclib combined with endocrine therapy for the adjuvant treatment of HR+, HER2−, node-positive, high-risk, early breast cancer (monarchE). J Clin Oncol. 2024;42(9):987–993. doi:10.1200/JCO.23.02338
Turner NC, Oliveira M, Howell SJ, et al. Capivasertib in hormone receptor-positive advanced breast cancer. N Engl J Med. 2023;388(22):2058–2070. doi:10.1056/NEJMoa2214131

 中文
中文 English
English 한국어
한국어 日本語
日本語 Español
Español Français
Français Русский
Русский